About Diskectomy
A diskectomy is a surgical procedure to remove the herniated portion of a spinal disc that's pressing on a nerve root. Unlike a complete disc removal, I remove only the fragment causing compression—preserving as much of your disc as possible. This targeted approach allows for faster recovery while effectively eliminating the radiating pain that conservative treatments couldn't address.
I perform diskectomy at my offices in both San Antonio and Houston, using advanced techniques I developed during my training at Mayo Clinic in orthopedic and neurosurgical spine surgery. My dual fellowship background gives me a unique precision in working near delicate nerve structures—I can remove the exact amount of disc material needed without unnecessary damage to surrounding tissues.
When Diskectomy Is Recommended
Diskectomy is most effective for radiating pain—the kind that shoots down your arm or leg—rather than localized back or neck pain alone. This happens when a herniated disc pushes through its outer layer and pinches a nerve root.
I recommend considering diskectomy when:
- You have persistent radiating pain that's interfering with work, sleep, or daily life
- Conservative treatments—physical therapy, medications, and injections—have failed to provide relief after several weeks
- You're experiencing significant weakness or loss of function in your arm or leg
- Imaging studies clearly show the herniated disc is causing your symptoms
The goal is to get you back to your life. I only recommend surgery when I'm confident it will make a real difference.
How I Perform Diskectomy
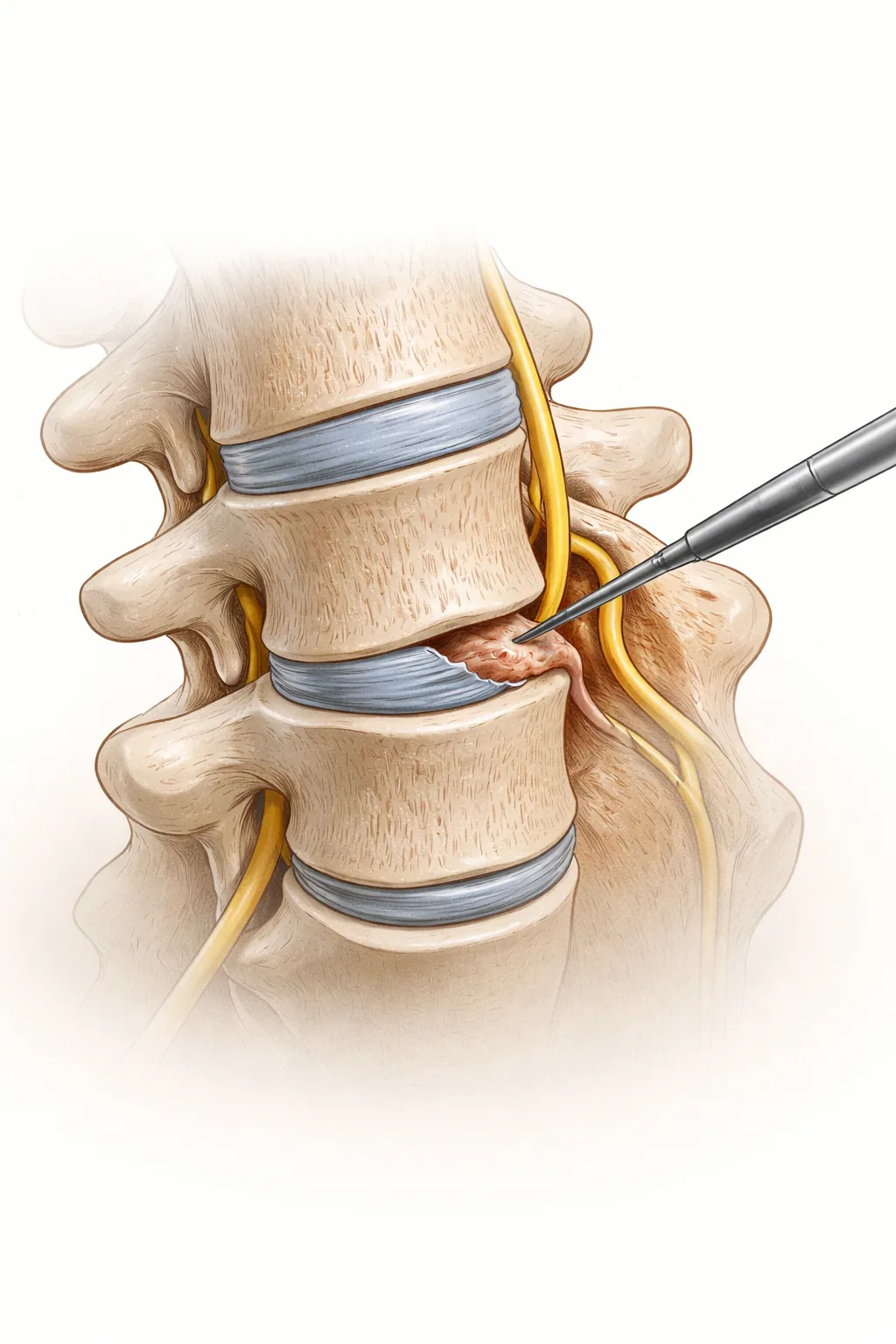
During the procedure, performed under general anesthesia, I make a small incision to access the herniated disc. I may remove a small amount of bone or ligament to reach the disc safely—similar to a laminectomy—but my focus is precise: I extract only the disc fragment that's pressing on the nerve.
Here's what's important to understand: I leave most of your disc intact. The nucleus pulposus—the gel-like center of the disc—remains unless it's the specific part causing nerve compression. This preservation approach supports better long-term stability.
In cases where imaging or intraoperative assessment reveals that your spine is unstable after disc removal, I may recommend fusion. I prefer using bone graft from a donor (allograft) rather than taking bone from your own body, which reduces operative time and eliminates donor-site pain.
What to Expect
Most diskectomy patients go home the same day or spend just one night in the hospital. You'll be under general anesthesia, so you'll need someone to drive you home and stay with you that first night.
Before surgery, you'll need to:
- Stop blood-thinning medications as directed
- Fast for 8 hours prior to your appointment
- Arrange easy-reach supplies at home (water, medications, phone, remote controls)
- Prepare meals in advance or have someone available to help
During recovery, walking is your best friend—it increases blood flow and reduces stiffness. For the first 6 weeks, limit heavy lifting to 5 pounds or less. Most patients return to light desk work within 2 to 4 weeks, though those in manual labor may need 4 to 6 weeks.
Recovery
The beauty of diskectomy is that it typically brings rapid symptom relief. Many patients notice improvement in radiating pain within days to weeks—far faster than conservative treatment would provide.
While diskectomy eliminates symptoms for most patients, it's not always permanent. Your remaining disc tissue can herniate again, though this happens in a minority of cases. I'll discuss realistic expectations during your consultation.
Throughout your recovery, I'm available at my San Antonio and Houston offices to monitor your progress, address any concerns, and ensure you're healing as expected.
Have questions about diskectomy or herniated discs? Schedule a consultation with Dr. Cyr at one of our San Antonio or Houston locations. We'll review your imaging, discuss your symptoms, and determine whether diskectomy is right for you.
Related: Learn more about herniated discs or lumbar fusion if your spine requires additional stabilization.
When This Procedure Is Recommended
- Radiating pain into arms, legs, buttocks, or chest
- Numbness and tingling in the extremities
- Muscle weakness or loss of strength
- Difficulty standing or walking for extended periods
- Pain that limits daily activities despite conservative treatment
Surgical Techniques
- Physical therapy and anti-inflammatory medication
- Epidural steroid injections
- Diskectomy surgery
- Lumbar or cervical fusion (if instability is present)
Frequently Asked Questions
How long is recovery after diskectomy surgery?
Most patients go home the same day or after one night in the hospital. You can return to light activities within 2–4 weeks. Many patients experience improvement in radiating pain within days to weeks.
Will my herniated disc come back after diskectomy?
For most patients, no. However, in a minority of cases, the remaining disc tissue can herniate again from the same level. Dr. Cyr discusses realistic expectations and alternatives during your consultation.
Why would I need fusion after diskectomy?
If imaging or intraoperative assessment reveals that your spine is unstable after disc removal, fusion may be recommended to stabilize the segment and prevent future problems.
What is the difference between diskectomy and laminectomy?
Diskectomy removes herniated disc material pressing on a nerve. Laminectomy removes bone (lamina) to enlarge the spinal canal. Both may be needed depending on what's causing your compression.
Can I lift and bend normally after diskectomy?
For the first 6 weeks, limit heavy lifting to 5 pounds or less. After healing, most patients return to normal activities including lifting and bending without restrictions.

