What Is a Herniated Disc?
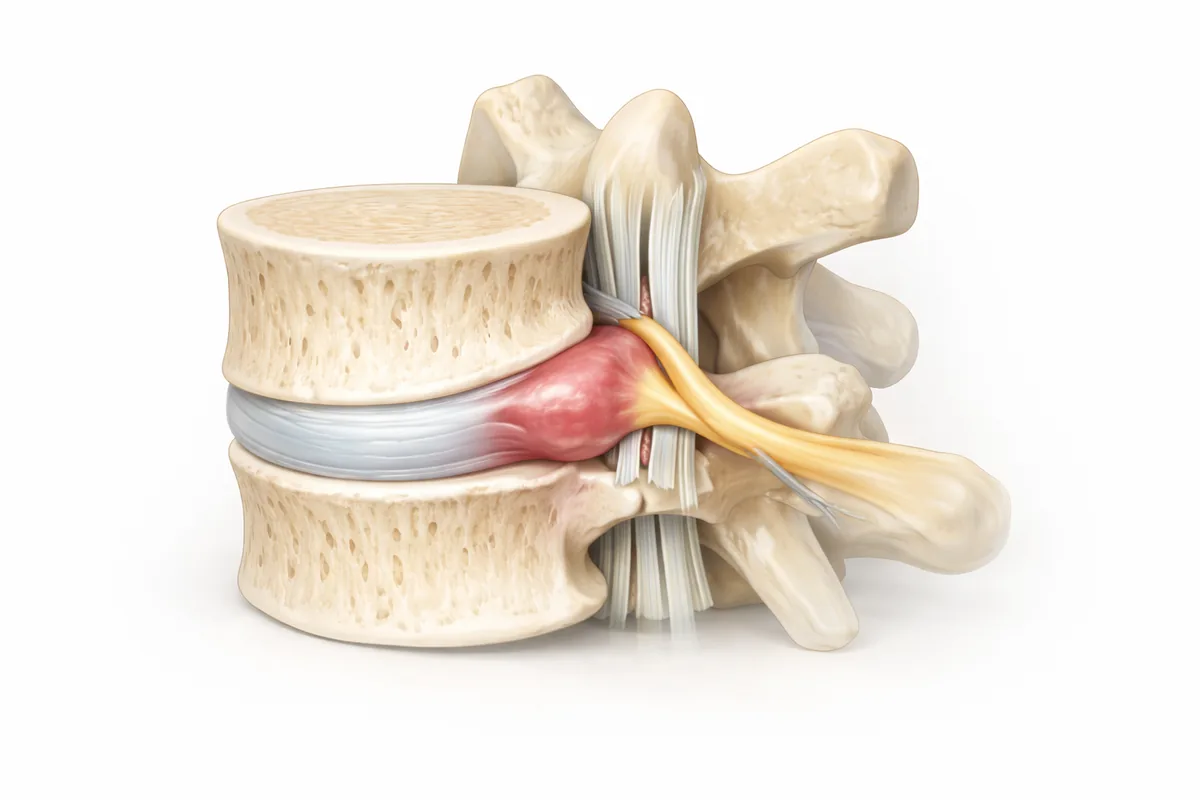
Your spinal discs act as shock absorbers between vertebrae—think of them as the spine's suspension system. Each disc has a tough outer layer (annulus fibrosus) and a soft gel-like center (nucleus pulposus). When the outer layer weakens or tears, that inner material can push through and compress nearby nerve roots or the spinal cord itself. That's a herniated disc, and it's one of the most common reasons patients come into my practice. When a lumbar disc herniates, the resulting nerve compression often produces sciatica—radiating pain down the leg that can be debilitating.
The herniation doesn't always happen suddenly. Often, it's years of degeneration, repetitive stress, or improper lifting mechanics that gradually compromise the disc. Sometimes a single awkward movement is the final straw. Either way, once that nerve is compressed, you typically feel it—and it can be quite painful.
Why Herniated Discs Happen
Age and degeneration are the primary culprits. As we get older, discs lose water content and flexibility, making them more prone to cracking. Unlike a bulging disc, where the disc extends uniformly beyond its normal boundary, a herniated disc involves a rupture that allows inner material to escape. By the time most of my patients reach their 40s and 50s, some disc degeneration is visible on imaging, even if they're asymptomatic.
Injury and strain accelerate the process. Heavy lifting with poor form, repetitive bending, or sudden trauma can tear the disc's outer layer. I see this often in people whose jobs involve manual labor or prolonged sitting.
Lifestyle factors matter too: smoking reduces disc nutrition, excess weight increases spinal load, and sedentary habits weaken the core muscles that stabilize your spine.
Genetics play a role. Some people inherit a predisposition to disc problems, which is why I ask detailed family history during initial consultations.
How I Diagnose a Herniated Disc
My diagnostic approach combines clinical examination with imaging. I start with a thorough history and physical exam—testing your strength, reflexes, and range of motion to pinpoint which nerve level is involved. I look for specific weakness patterns and pain patterns that tell me exactly where the problem is.
MRI is my gold standard. It shows the disc, the spinal cord, nerves, and any inflammation with excellent soft-tissue detail. I can see exactly how large the herniation is, in what direction it's pointing, and whether it's actually compressing a nerve or just sitting there.
CT imaging is helpful when MRI isn't possible or when I need to assess bone detail for surgical planning. Sometimes a combination of both gives me the clearest picture.
Imaging is only one piece of the puzzle, though. I've seen patients with huge herniations on MRI but minimal symptoms, and others with small herniations causing severe pain. The clinical correlation—matching the imaging to your specific symptoms—is what guides my recommendations.
Conservative Treatment: Where Most Cases Start
The vast majority of herniated discs respond well to non-surgical care, and that's always my first-line approach. You don't need surgery just because you have a herniated disc.
Physical therapy is the cornerstone. A good spine PT program focuses on core stabilization, gentle stretching, and movement retraining. Your core muscles—the deep abdominals and back extensors—are your spine's natural support system. Strengthening them takes pressure off the disc and protects against re-injury.
Anti-inflammatory medications like NSAIDs and short courses of muscle relaxers can help manage pain and allow you to participate in PT more effectively. I often combine this with activity modification: avoiding the movements that triggered your pain while gradually returning to normal function.
Epidural steroid injections are very effective for many patients, especially those with nerve root irritation. The steroid reduces inflammation around the nerve, which can provide relief for weeks or months and give PT time to work. I typically recommend up to three injections in a rolling 12-month period—beyond that, we're looking at diminishing returns.
Rest and time matter. Many disc herniations gradually shrink as the body reabsorbs the extruded material, especially in younger patients. Giving your spine time to heal while you're in PT is reasonable.
Most patients feel significantly better within 6-12 weeks of consistent conservative care. The key word is consistent—you have to do your PT, modify your activities, and give it time.
When Surgery Becomes Necessary
I recommend surgical intervention when:
- Conservative care fails: You've done 6-12 weeks of PT, injections have lost effectiveness, and you're still significantly limited
- Neurologic compromise is progressive: Your weakness is getting worse despite treatment, which can mean permanent nerve damage is imminent
- Bowel or bladder dysfunction develops: This is cauda equina syndrome, a surgical emergency
- Pain is intolerable: Life quality is severely compromised despite medical management
Fusion is my preferred surgical approach for symptomatic herniated discs. Unlike simple discectomy (removing disc material), fusion stabilizes the spine long-term by joining the vertebrae above and below the problem disc. This prevents future problems at that level and gives you the most durable result. I'll remove the herniated disc material and then fuse the vertebrae using bone graft and instrumentation (plates, screws).
For cases with associated stenosis—where the spinal canal is narrowed—I often perform a laminectomy-fusion, removing the back of the vertebra to decompress the spinal cord or nerve roots while fusing for stability.
The advantage of fusion is permanence. Recurrent herniations at the same level are rare after fusion. Some surgeons advocate for simple discectomy without fusion, but my training and experience have convinced me that fusion provides superior long-term outcomes and patient satisfaction, particularly in my patient population where we're trying to prevent future surgeries.
What to Expect From Surgery
My fusion procedures are typically minimally invasive when possible. I discuss exact approaches and recovery timelines during your consultation—it varies depending on whether your herniation is cervical, thoracic, or lumbar.
Recovery is measured in weeks and months, not days. Most patients are back to light activity in 4-6 weeks, gradually advancing from there. I'm conservative with returning to heavy lifting or high-impact activities—usually 3-4 months before unrestricted activity.
Serious complications are rare, but any surgery carries some risk. During your consultation, I'll discuss complications specific to your situation in detail.
Related Conditions & Treatments
- Bulging Disc: How It Differs
- Sciatica & Sciatic Nerve Pain
- Pinched Nerve Treatment
- Herniated Disc Specialist — When to Seek Care
- Diskectomy Surgery
- Microdiscectomy vs. Fusion
- Lumbar Fusion Surgery
Next Steps
If you're dealing with back or neck pain from a suspected herniated disc, don't assume you need surgery. My role is to guide you through the diagnostic process and create a treatment plan tailored to your imaging, your symptoms, and your goals.
Many patients do beautifully with conservative care. For those who need surgery, I'm here with expertise and experience to make it count.
Schedule a consultation at my San Antonio or Houston office. We'll image your spine, examine you carefully, and build a clear path forward—whether that's PT, injections, surgery, or a combination approach.
Your spine is complex. Your treatment shouldn't be generic.
Common Symptoms
- Localized back or neck pain at the affected level
- Radiating pain down the arm (cervical) or leg (lumbar)
- Numbness or tingling in the distribution of the compressed nerve
- Weakness in muscles supplied by the affected nerve
- Difficulty with fine motor control (grip strength, dexterity)
- Pain that worsens with certain movements or positions
- Muscle spasm or stiffness around the herniated disc
Treatment Options
- Physical therapy and targeted core strengthening
- Anti-inflammatory medications (NSAIDs, muscle relaxers)
- Epidural steroid injections for nerve inflammation
- Cervical or lumbar fusion for persistent symptoms
- Laminectomy-fusion for cases with stenosis
- Activity modification and postural correction
- Weight management to reduce spinal load
Frequently Asked Questions
Do all herniated discs require surgery?
No. Most herniated discs respond well to conservative treatment including physical therapy, medications, and injections. Dr. Cyr recommends surgery only when conservative care fails or neurological symptoms progress.
How long does it take a herniated disc to heal?
Most patients experience significant improvement within 6-12 weeks of consistent physical therapy. The body gradually reabsorbs disc material, especially in younger patients. Recovery time depends on the severity and your adherence to conservative care.
Can I get herniated disc treatment in San Antonio?
Yes. Dr. Cyr offers comprehensive herniated disc evaluation and treatment at his San Antonio office (8401 Datapoint Drive). He provides both conservative care coordination and surgical options when needed.
What's the difference between a herniated disc and a bulging disc?
A herniated disc has a rupture in the outer layer allowing inner material to leak out, often causing acute symptoms. A bulging disc extends uniformly outward without rupture. Herniated discs typically cause sharper, more immediate pain.
Will MRI confirm my herniated disc diagnosis?
MRI is the gold standard for diagnosing herniated discs, showing the exact location, size, and whether it's compressing a nerve. However, imaging must correlate with your specific symptoms to guide treatment decisions.

