What Is Sciatica?
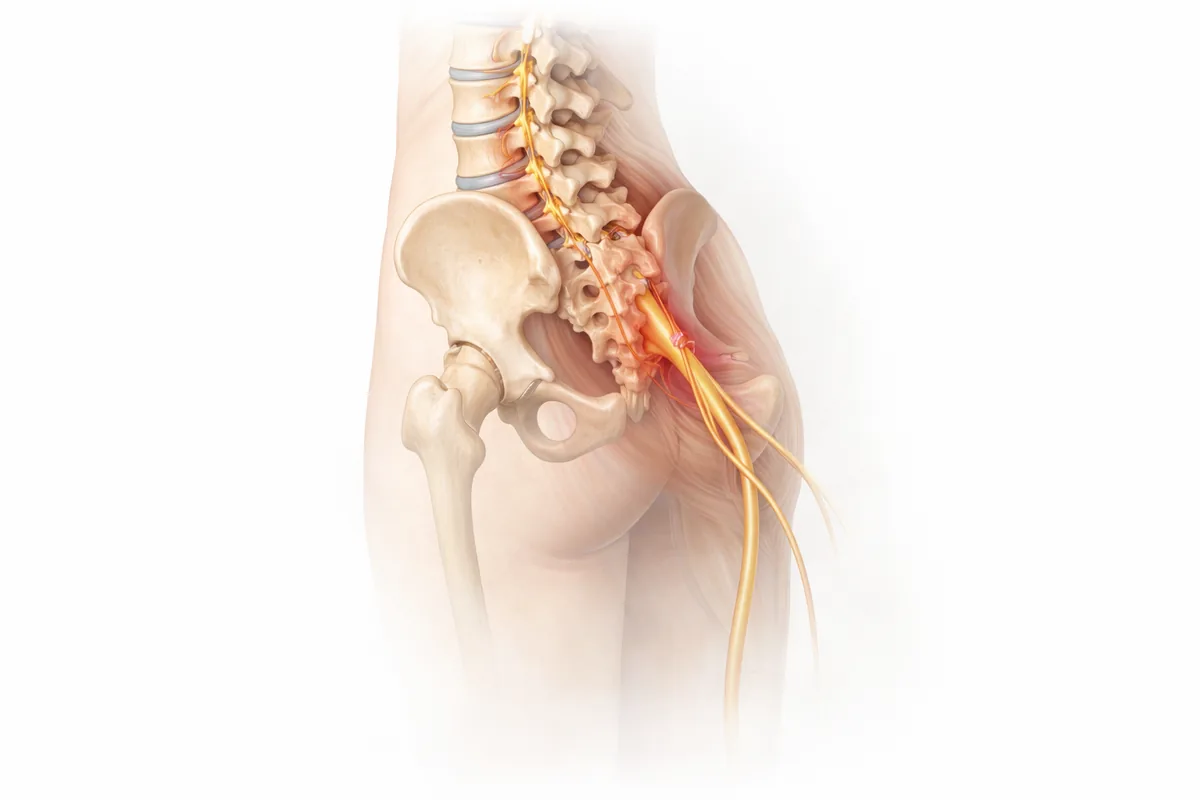
Sciatica is pain that radiates along the sciatic nerve—the longest nerve in your body, running from your lower back through your buttocks and down each leg. When something compresses this nerve, you feel characteristic pain that shoots down the back of your leg, often accompanied by numbness, tingling, or weakness.
The key word is compression. The sciatic nerve gets pinched at its origin in the lower spine, and that compression sends pain signals all the way down the distribution of the nerve. It's one of the most common reasons patients end up in my clinic describing burning leg pain or numbness in their foot—and it's often very treatable.
What Causes Sciatic Nerve Compression
The sciatic nerve emerges from the lumbar spine at L4-S1 nerve roots. Several spinal conditions can compress it:
Herniated disc in the lumbar spine is the most common culprit. When a disc herniates in the lower back, the protruding material can push directly on the nerve root, causing immediate inflammation and pain down the leg.
Bone spurs (osteophytes) develop from osteoarthritis or degenerative disc disease. These bony growths encroach into the nerve canal, gradually narrowing the space where the nerve travels.
Lumbar stenosis is a narrowing of the spinal canal itself, often from a combination of degenerative changes—disc bulging, thickened ligaments, and facet joint arthritis. The nerve doesn't have enough room, and symptoms develop.
Spondylolisthesis (vertebral slippage) misaligns the vertebrae, which can stretch or compress the emerging nerve root.
Foraminal stenosis occurs when the neural foramen—the small opening where the nerve exits the spine—narrows, compressing the nerve root right at its exit point. This is a particularly common pattern I see in my patients.
Tight piriformis muscle syndrome is less common but worth knowing: the sciatic nerve can be compressed as it passes under the piriformis muscle in the buttock, even without spine involvement.
Age, degenerative changes, prior injury, and repetitive strain all increase your risk. Prolonged sitting—especially in poor posture—loads the lumbar spine and can aggravate existing nerve compression.
How I Diagnose Sciatica
My diagnostic approach identifies not just that you have sciatica, but why you have it and which nerve root is affected. The treatment depends on the underlying cause.
Clinical examination comes first. I perform specific tests: straight leg raise (pain radiating below the knee strongly suggests nerve root involvement), crossed straight leg raise, manual muscle testing, and reflex testing. The pattern of weakness and numbness tells me exactly which nerve root—L4, L5, or S1—is compressed.
MRI imaging is the gold standard. It shows me the disc, spinal canal, nerve roots, and any structural narrowing or compression with excellent detail. I can see whether you have a herniated disc, stenosis, bone spurs, or foraminal narrowing—and exactly where the nerve is getting squeezed.
Clinical correlation is essential. I've seen patients with incidental findings on MRI that aren't the actual source of their pain. That's why the physical exam—matching imaging to your specific symptoms—guides my recommendations.
Conservative Treatment: The First Step
Most sciatica cases respond well to non-surgical care, and that's my starting point for nearly every patient. Surgery is reserved for those who fail conservative therapy or have progressive neurological compromise.
Physical therapy is foundational. A sciatic-focused PT program emphasizes:
- Nerve mobility work: Specific stretches like nerve flossing help the sciatic nerve move freely through the pelvis and lower spine without getting tethered.
- Core stabilization: Strong deep abdominals and multifidus muscles support the lower spine and take pressure off compressed nerve roots.
- Hip flexibility: Tight hip muscles, especially the piriformis, can contribute to nerve compression. Targeted stretching addresses this.
- Postural retraining: Many patients have movement habits that worsen compression—I work with PT to break those patterns.
Most patients feel significant improvement within 4-8 weeks of consistent PT, especially when combined with other conservative measures.
Anti-inflammatory medications including NSAIDs and short-term muscle relaxers can reduce inflammation around the compressed nerve and allow better participation in PT. I rarely prescribe long-term opioids for sciatica—they mask the problem without treating it.
Epidural steroid injections are particularly effective for sciatica. The steroid is delivered directly into the epidural space around the compressed nerve root, reducing inflammation and providing relief. Many of my patients get significant pain reduction for weeks or months, giving PT time to strengthen supporting muscles. I typically recommend up to three injections spaced 2-3 weeks apart if the first is helpful—after that, diminishing returns usually set in.
Activity modification is critical. I counsel patients to avoid or modify movements that trigger pain—prolonged sitting, heavy lifting, repetitive bending—while maintaining gentle mobility to prevent stiffness.
Time and rest matter. Many disc herniations gradually reabsorb, and inflammation naturally decreases with relative rest and conservative care. Patience and consistency are your allies.
When Surgery Becomes Necessary
I recommend surgical intervention for sciatica when:
- Conservative therapy fails after 8-12 weeks: You've done physical therapy, tried injections, modified activities, and you're still significantly limited in function and quality of life
- Neurological deficit progresses: Your leg weakness is worsening despite non-surgical treatment, signaling risk of permanent nerve damage
- Severe or intractable pain impairs function: Your pain is so severe that you cannot work, care for yourself, or participate meaningfully in daily life despite medical management
- Acute cauda equina syndrome: Bowel or bladder dysfunction, bilateral leg pain, or progressive bilateral weakness require urgent decompression—this is a surgical emergency
Surgical Options: Decompression and Fusion
When surgery is indicated, my approach depends on the underlying pathology.
Laminectomy is the most direct approach for nerve root compression. I remove the lamina (back portion of the vertebra) to decompress the nerve root at its exit point. This is particularly effective for foraminal stenosis, where the nerve is pinched right at the neural foramen. For a single-level stenosis causing sciatica, laminectomy alone often provides durable relief.
Laminectomy-fusion is my choice when the underlying cause involves instability—a slipped vertebra, significant disc degeneration causing hypermobility, or if you've had prior spine surgery at that level. Fusion stabilizes the segment after decompression, preventing future compression and providing more durable results. I perform minimally invasive fusion using pedicle screws and bone graft, which preserves muscle and shortens recovery.
Nerve block or transforaminal epidural approaches are sometimes helpful preoperatively or if you want to confirm the nerve root is truly the source of pain—but once surgical indication is clear, decompression is definitive.
My Philosophy on Sciatica Surgery
I've trained extensively in both orthopedic and neurosurgical spine techniques, which gives me deep expertise in nerve decompression. My approach is conservative: I don't operate until conservative care has been genuinely exhausted, and when I do operate, I decompress thoroughly—removing all bony and soft-tissue sources of compression—and fuse when appropriate to prevent recurrence.
The goal is to get you back to your life, free of radiating leg pain, with confidence that your symptoms won't return.
What to Expect From Decompression Surgery
Laminectomy-fusion is typically performed under general anesthesia. I position you prone, use real-time fluoroscopy to guide placement, and make small incisions over the affected segment. I remove the lamina to open up the spinal canal, remove any disc material or bone spurs compressing the nerve, and visualize the nerve decompression directly. If fusion is needed, I place pedicle screws and a rod to stabilize the segment.
Most procedures take 1-2 hours per level. Many patients go home the same day; some stay overnight for observation.
Recovery after minimally invasive laminectomy-fusion is faster than traditional open surgery:
- Weeks 1-2: Rest, frequent short walks, pain management. Avoid bending and heavy lifting.
- Weeks 2-6: Gradual increase in activity under brace support. PT can begin.
- Weeks 6-12: Progressive strengthening, return to light activities. Most patients resume desk work around 4-6 weeks.
- Months 3-6: Return to normal activities, exercise, and full work duties. Nerve healing may continue improving for several months.
Related Conditions & Treatments
- Herniated Disc Treatment
- Lower Back Pain
- Pinched Nerve Treatment
- Spinal Stenosis
- Lumbar Spine Surgery
- Laminectomy with Fusion
Next Steps
If you're experiencing sciatic nerve pain—radiating leg pain, numbness, or weakness—don't resign yourself to chronic pain. Modern conservative care and surgical decompression are highly effective.
My approach is individualized: we image your spine, examine you thoroughly, and build a treatment plan based on your specific anatomy, symptoms, and goals. Many patients improve dramatically with non-surgical care. Those who need surgery get the benefit of expert decompression with minimal trauma and rapid recovery.
Schedule a consultation at my San Antonio or Houston office. We'll determine exactly what's compressing your nerve and chart the best path to relief.
Your sciatic nerve pain doesn't have to be permanent. Let's fix it.
Common Symptoms
- Sharp or burning pain radiating from the lower back through the buttock down one leg
- Numbness or tingling sensation in the leg, foot, or toes
- Weakness in the leg, difficulty lifting the foot or walking
- Pain worse when sitting, especially for prolonged periods
- Pain that worsens with certain movements like bending forward
- Difficulty with bowel or bladder control (rare but urgent)
- Muscle weakness or atrophy in advanced cases
Treatment Options
- Physical therapy focusing on nerve mobility and core strength
- Anti-inflammatory medications and pain management
- Epidural steroid injections to reduce nerve inflammation
- Activity modification and postural correction
- Nerve decompression surgery (laminectomy, foraminotomy)
- Lumbar fusion for cases with instability or recurrent compression
Frequently Asked Questions
What causes sciatica pain down my leg?
Sciatica occurs when the sciatic nerve is compressed at its origin in the lower spine, usually by a herniated disc, bone spurs, or narrowing of the spinal canal. The compression causes pain that radiates along the nerve pathway.
How long does sciatica typically last?
Most sciatica cases improve significantly within 4-8 weeks of consistent physical therapy and conservative treatment. Some patients recover in weeks, while others may take 3-6 months for complete resolution.
Where can I get sciatica treatment in San Antonio and Houston?
Dr. Cyr specializes in sciatica treatment at both locations—San Antonio office (8401 Datapoint Drive) and Houston office (9125 West Road). He offers nerve decompression surgery when conservative care doesn't provide relief.
Will physical therapy cure my sciatica?
Physical therapy is highly effective for sciatica. A program focusing on nerve mobility, core strengthening, and hip flexibility helps most patients achieve significant relief, especially when combined with activity modification and injections if needed.
When is sciatica surgery necessary?
Surgery is considered after 8-12 weeks of unsuccessful conservative treatment, or when neurological symptoms progressively worsen. Progressive weakness or bowel/bladder dysfunction require urgent evaluation.

