About the Procedure
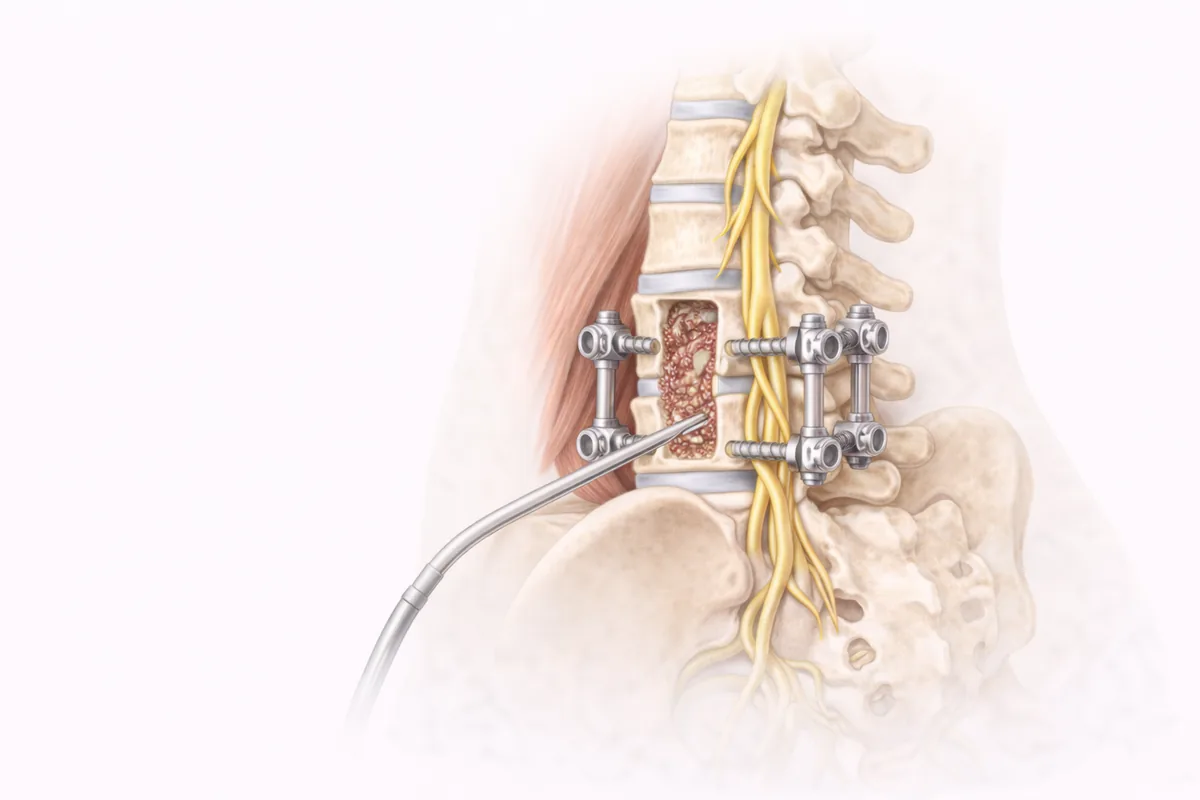
Laminectomy with fusion is a surgical approach that addresses two distinct problems: removing pressure from compressed nerves and stabilizing the spine where instability exists. During the procedure, I remove the lamina—the back portion of one or more vertebrae—to enlarge the spinal canal and relieve pressure on the spinal cord or nerve roots. When spinal instability is present, I then perform a fusion, connecting adjacent vertebrae with bone graft and instrumentation to restore structural integrity.
This is fundamentally different from simple decompression alone. In my practice across San Antonio and Houston, I've found that combining decompression with fusion produces superior long-term outcomes for patients with significant stenosis accompanied by instability or scoliosis. My Mayo Clinic training—specifically my combined fellowship in both orthopedic and neurosurgical spine—gives me the technical skill to approach these challenging cases from multiple angles and choose the most appropriate strategy for each patient's anatomy.
When Surgery Is Recommended
Laminectomy with fusion is considered only after conservative treatments have proven insufficient. I typically recommend this procedure when imaging confirms significant spinal canal narrowing or nerve root compression, and the patient's symptoms correlate with those findings.
You may be a candidate for this surgery if you have:
- Spinal stenosis causing leg pain or walking difficulties
- Degenerative disc disease with secondary stenosis and neural element compression
- Disc herniation pressing on nerves, causing radiculopathy
- Spondylolisthesis (vertebral slippage) creating instability and nerve pressure
- Neurological symptoms—numbness, weakness, or loss of bladder/bowel control—that suggest urgency
Before recommending surgery, I ensure that non-surgical options have been exhausted: physical therapy, medications, targeted injections, and activity modification. I also confirm that you're medically appropriate for surgery and have adequate support during recovery.
Dr. Cyr's Approach
In my experience, success in laminectomy with fusion depends on precise surgical technique and careful patient selection. I approach each case individually, determining exactly how much decompression is needed without over-resecting bone, which can compromise stability.
Surgical Decision-Making
I use advanced imaging and physical examination to identify not just where the compression is, but whether fusion is truly necessary. Not every decompression requires fusion. However, when I detect instability—either from significant degenerative changes, previous surgery, or scoliosis—I add fusion to prevent recurrent stenosis and long-term pain. The fusion approach may involve lumbar fusion techniques depending on the spinal levels affected and your anatomy.
Technical Precision
My training allows me to work safely near the spinal cord and nerve roots while maximizing decompression. I use intraoperative monitoring when appropriate to confirm nerve function throughout the procedure. For fusion, I select the approach—posterior, anterior, or combined—that best addresses your specific pathology while minimizing tissue trauma.
Instrumentation
When fusion is necessary, I use modern instrumentation systems that provide immediate stability while allowing natural bone fusion to develop. This approach reduces complications and speeds recovery compared to older techniques.
What to Expect
Before Surgery
I'll see you in my San Antonio or Houston office for pre-operative evaluation, imaging review, and discussion of your specific case. I answer all questions thoroughly—this is major surgery, and you should feel completely confident in the plan.
During Surgery
The procedure typically takes 2–4 hours, depending on the number of levels treated and whether fusion is performed. You'll receive general anesthesia. I make an incision along the midline of your back, exposing the lamina and underlying structures. After careful decompression, I remove any disc material pressing on nerves, then perform the fusion if indicated, securing it with bone graft and instrumentation.
Hospital Stay
Most patients stay 1–3 days in the hospital after fusion surgery. You'll wake up in the recovery room, and my team will manage pain aggressively so you can begin moving safely within hours.
Recovery
Early Recovery (Weeks 1–4)
You'll work with physical therapy to learn proper body mechanics—how to get out of bed, walk, and sit without straining the fusion. I typically recommend:
- No twisting, bending, or heavy lifting for at least 6 weeks
- Gradual increase in walking as tolerated
- Pain management with prescribed medications as needed
- Wearing a back brace or support if recommended
Progressive Recovery (Weeks 4–12)
As pain decreases, you'll gradually increase activity. Formal physical therapy focuses on core strengthening, flexibility, and functional movement. Most patients return to light duty work by 6–8 weeks and resume normal activities by 3–4 months.
Long-Term Outcomes
Studies consistently show that laminectomy with fusion provides durable relief of neurological symptoms—the numbness, weakness, and pain caused by nerve compression—in the majority of patients. The fusion protects against recurrent stenosis at that level, though degenerative changes can occasionally occur at adjacent levels years later.
I typically see patients at 2 weeks, 6 weeks, 3 months, and 1 year post-operatively. This follow-up ensures you're progressing appropriately and addresses any concerns early.
Risks and Complications
Like all spine surgery, laminectomy with fusion carries standard surgical risks: infection, bleeding, blood clots, and fluid leaks. Nerve or spinal cord injury is rare but possible. Additional risks specific to fusion include non-union (failure of bones to fuse), implant complications, and adjacent-segment degeneration.
I discuss your individual risk profile during consultation, particularly if you have diabetes, heart disease, smoking history, or previous spine surgery—all factors that can affect healing.
If you're experiencing persistent back or leg pain, numbness, or weakness despite conservative treatment, I invite you to schedule a consultation at my San Antonio or Houston office. Together we'll determine whether laminectomy with fusion is right for you.
When This Procedure Is Recommended
- Chronic back or neck pain unresponsive to conservative treatment
- Numbness, tingling, or weakness in the arms, hands, legs, or feet
- Pain radiating along the sciatic nerve or down the extremities
- Loss of fine motor control or coordination
- Neurological symptoms from spinal cord or nerve compression
- Difficulty walking or standing for prolonged periods
Surgical Techniques
- Decompressive Laminectomy
- Laminotomy with targeted nerve decompression
- Spinal fusion with instrumentation
- Posterior fusion approaches
- Combined anterior-posterior fusion when indicated
Frequently Asked Questions
How long does recovery from laminectomy with fusion take?
Most patients return to light activities within 4–6 weeks. Full fusion typically occurs over 3–6 months, during which Dr. Cyr monitors your progress with follow-up imaging. Most restrictions lift by 3 months.
Will I lose flexibility after spinal fusion?
Fusion eliminates motion at the treated level, but most patients notice minimal impact on daily activities. Adjacent segments continue to provide movement and flexibility, and physical therapy helps restore functional motion.
When is fusion necessary with laminectomy?
Fusion is added when your spine shows instability from degeneration, scoliosis, spondylolisthesis, or previous surgery. Not every laminectomy requires fusion—Dr. Cyr determines this based on your specific anatomy and imaging.
What is the difference between laminectomy alone and laminectomy with fusion?
Laminectomy removes bone to decompress nerves. Fusion adds stabilization by connecting vertebrae together. Laminectomy alone works when stenosis is the only problem; fusion is added when instability also exists.
What happens to adjacent discs after fusion?
Adjacent discs bear slightly more load after fusion, and degenerative changes can rarely develop at those levels years later. However, maintaining core strength and good posture significantly reduces this risk.

