What Is Microdiscectomy?
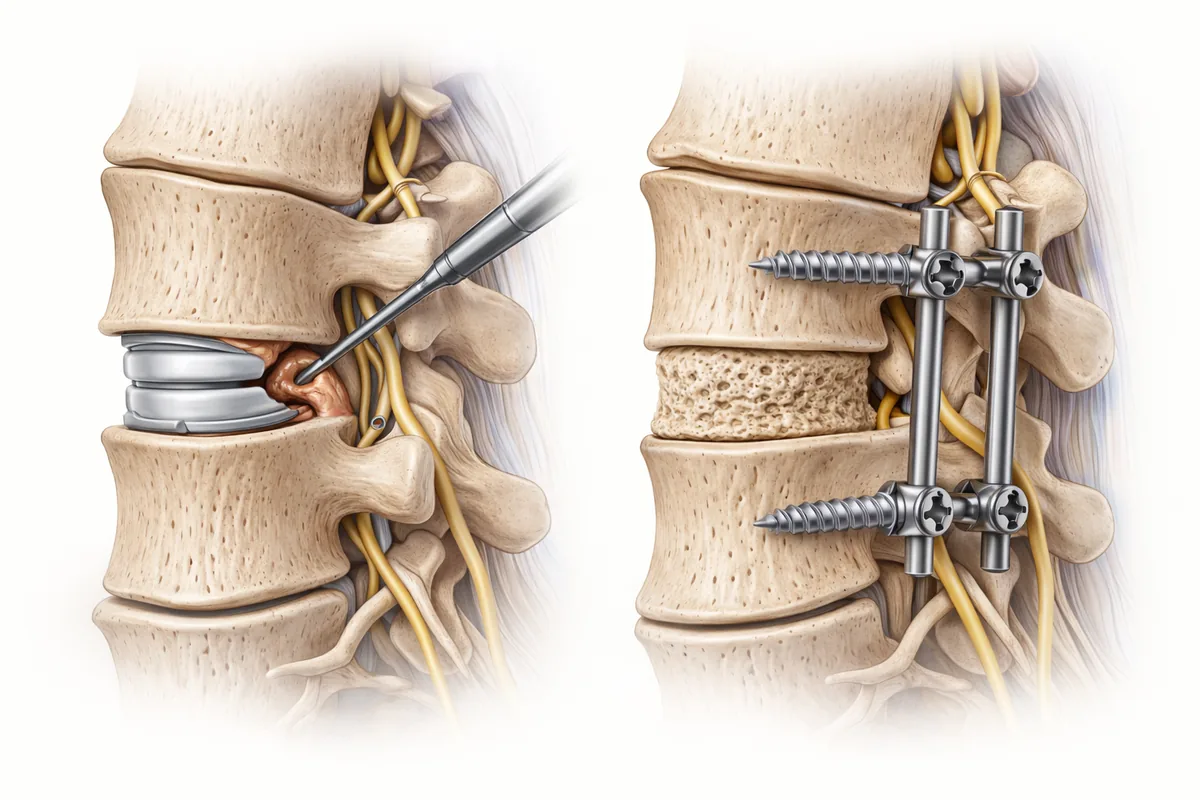
Microdiscectomy is a minimally invasive surgical procedure designed to remove herniated disc material pressing on a nerve. The surgeon makes a small incision and uses magnification or an endoscope to carefully extract only the bulging or fragmented portion of the disc, leaving the disc structure itself largely intact.
The procedure typically takes about an hour under general anesthesia. It can be performed endoscopically (through a tiny camera and instruments), through a mini-open approach, or using a tubular retractor system. Recovery is faster than traditional open surgery, and patients often go home the same day.
On the surface, this sounds appealing. But after performing hundreds of spine surgeries and training at Mayo Clinic, I've learned that removing just the fragment is not the answer to the underlying problem.
The Re-Herniation Problem
Here's the hard truth: the disc material returns in a significant percentage of patients. Studies show that re-herniation rates after microdiscectomy range from 5–20% — and those are conservative estimates in some patient populations.
When a disc herniates once, it's because the disc structure itself is compromised. The outer layers have weakened, and the inner nucleus has lost its integrity. Simply removing the piece of disc that's pressing on the nerve doesn't address this fundamental problem. You've removed the symptom, but you've left the broken disc in place.
What happens next? Months or years later — sometimes within weeks — more disc material herniates from the same level. Suddenly, the patient is back in my office with renewed pain and radiculopathy, now facing the choice between another microdiscectomy (which has even lower success rates the second time) or the fusion they should have had in the first place.
I've seen this pattern too many times. The patient undergoes a "quick" procedure, gets temporary relief, and then requires a more extensive fusion surgery anyway — along with all the recovery time and disruption that comes with it.
Why I Choose Fusion Instead
Fusion solves the problem at its root. By removing the damaged disc and fusing the vertebrae together, we eliminate the source of instability. The adjacent levels stabilize, the nerve decompression is durable, and the risk of re-herniation at that level drops dramatically.
Yes, fusion is a more significant procedure. Yes, recovery takes longer. But I'm thinking about what's best for you five, ten, and twenty years down the road — not just the next three months.
My approach uses proven techniques like anterior cervical discectomy and fusion (ACDF), lumbar interbody fusion, or motion-preserving disc replacement when appropriate. The goal is the same: a definitive solution that allows you to return to function without the fear of a recurring herniation.
I also consider the biomechanics carefully. A fused segment changes how stress is distributed to adjacent discs, which is why careful patient selection and surgical technique matter. Done well, fusion is not a limiting procedure — it's a liberating one.
What This Means for You
If you're a candidate for surgery due to herniated disc symptoms that haven't responded to conservative care, my recommendation will be guided by your specific anatomy, your age, your activity level, and your long-term goals — not by the popularity of a procedure.
Microdiscectomy has a place in spine surgery, but not in my practice. I've chosen to focus on techniques that deliver durable results and reduce the likelihood of a second surgery.
That doesn't mean I'm dismissing surgeons who perform microdiscectomy. They may achieve good results in carefully selected patients. But I've found that fusion — done thoughtfully and with proper patient selection — is the more reliable path to long-term relief.
Next Steps
If you're dealing with arm or leg pain from a herniated disc, the first step is conservative treatment: physical therapy, anti-inflammatory management, and possibly targeted injections. Most herniated discs improve without surgery.
If conservative care hasn't worked after 6–12 weeks, and imaging confirms nerve compression, then surgery becomes the right option. At that point, I'll discuss fusion-based approaches designed to give you lasting relief.
Schedule a consultation to discuss your specific situation and explore the best surgical option for your spine health.
Related Reading:
- Herniated Disc: Symptoms and Treatment Options
- Diskectomy: Removing Disc Material
- Lumbar Fusion for Lasting Relief
When This Procedure Is Recommended
- Radiating arm or leg pain from a herniated disc
- Numbness or tingling in the extremities
- Weakness in arms or legs
- Pain that persists despite conservative treatment for 6-12 weeks
- MRI confirmation of herniated disc compressing a nerve
Surgical Techniques
- Anterior Cervical Discectomy and Fusion (ACDF)
- Lumbar Fusion
- Cervical Disc Replacement
- Non-surgical management with injections and physical therapy
Frequently Asked Questions
What is the re-herniation problem with microdiscectomy?
Studies show re-herniation rates after microdiscectomy range from 5–20%. Removing just the herniated fragment doesn't fix the underlying compromised disc. Months or years later, more disc material can herniate from the same level.
Why does Dr. Cyr recommend fusion instead of microdiscectomy?
Fusion permanently stabilizes the damaged disc by eliminating motion at that level. It addresses the root problem rather than just the symptom. Fusion has proven long-term durability and lower rates of recurrent symptoms.
Isn't fusion a more invasive procedure than microdiscectomy?
Yes, fusion is more significant surgery with longer recovery. However, fusion prevents the need for re-operation. One larger recovery is often better than two smaller recoveries separated by years of pain.
What happens if microdiscectomy fails and I need fusion later?
If microdiscectomy results in re-herniation, you'll face the choice between another microdiscectomy (with even lower success rates) or fusion. Having fusion done correctly the first time avoids this scenario.
Can I return to normal activities after fusion for a herniated disc?
Yes. After healing and physical therapy, most fusion patients return to normal daily activities and work. The fused segment no longer moves, but your spine adapts well and function is not limited.

