What Is Spinal Stenosis?
Spinal stenosis is a narrowing of the spinal canal—the tunnel through which your spinal cord and nerve roots travel. When this canal gets too tight, the structures inside get compressed, leading to pain, numbness, weakness, and in severe cases, neurological damage.
Think of your spine as a highway. In stenosis, the road narrows. If the narrowing is mild, traffic still flows. But as the canal gets tighter, even normal activity creates congestion and congestion creates symptoms.
The stenosis can develop in different parts of the spine: lumbar stenosis (lower back) is most common, affecting about 4–5% of the population, particularly as we age. Cervical stenosis (neck) is less common but more serious if severe, because the spinal cord itself is involved rather than individual nerve roots.
This is one of the most frequent conditions I treat, particularly in patients over 60. The good news: modern treatment—conservative care and carefully timed surgery—works extremely well.
Why Stenosis Develops
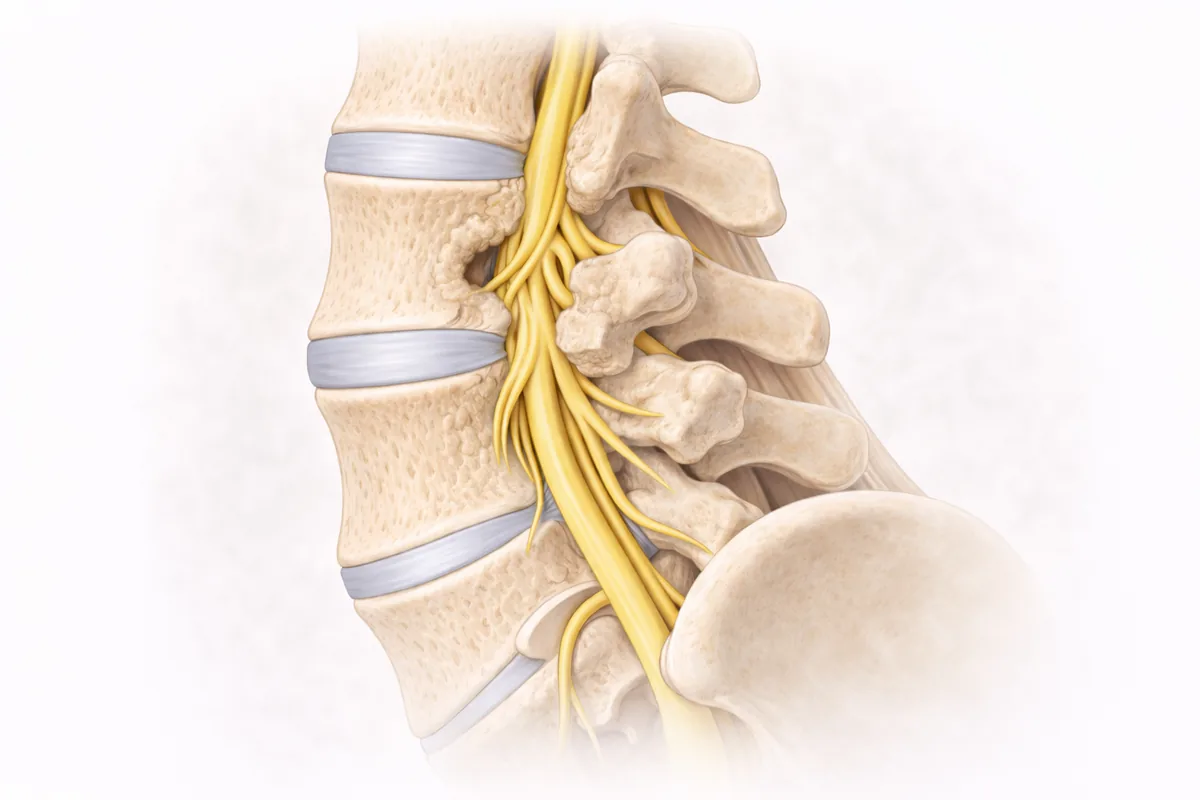
Spinal stenosis typically develops gradually over years through degenerative changes:
Disc bulging is usually the starting point. As discs lose hydration and flexibility with age, they bulge backward into the spinal canal. Unlike a herniated disc (where material ruptures out), bulging is more like a tire that's losing air—the disc loses height and its material presses into the canal.
Bone spurs (osteophytes) form along facet joints as the spine tries to stabilize itself through arthritic changes. These bony growths encroach into the canal from the sides and back.
Ligamentum flavum thickening happens as the spinal ligaments lose elasticity and thicken over time, further narrowing the canal from behind.
Facet joint arthritis causes the joints at the back of the spine to enlarge, and this also narrows the canal.
Spondylolisthesis (vertebral slippage) can narrow the canal by misaligning one vertebra relative to another, crushing the nerve roots between them.
These changes often develop together—a combination of disc bulging, bone spurs, and ligament thickening creates progressively tighter stenosis.
Age is the biggest risk factor. By your 70s, some degree of degenerative stenosis is visible on imaging in most people. Most remain asymptomatic, but when symptoms do develop, they can be quite limiting.
Prior injury or repeated stress accelerates degenerative changes. I see stenosis develop faster in patients with a history of disc herniation, trauma, or certain occupations.
The Classic Symptom Pattern
The most distinctive symptom pattern—neurogenic claudication—is called the "shopping cart sign." Patients experience burning leg pain, heaviness, or fatigue that worsens as they walk but improves dramatically when they sit down, lean forward, or bend at the waist. Many patients report they can walk longer distances if they lean on a shopping cart.
Why? When you sit or bend forward, you're opening up the spinal canal—relieving pressure on the compressed nerves. When you stand and walk straight upright, the canal narrows further and symptoms worsen.
Other common symptoms include:
- Numbness or tingling in the legs, buttocks, or feet
- Leg weakness or difficulty walking normally
- Loss of balance or unsteadiness
- Pain radiating into one or both thighs or calves
- For cervical stenosis: neck pain, stiffness, or pain radiating into the arms
- For severe cervical stenosis: hand weakness, difficulty with fine motor tasks, or balance problems (myelopathy)
One important distinction: some stenosis causes pain that radiates like sciatica, while other stenosis causes diffuse leg heaviness without true radicular pain. Understanding your specific symptom pattern helps me identify the exact level and type of stenosis.
How I Diagnose Spinal Stenosis
My diagnostic approach is both clinical and imaging-based—and they must correlate. I've seen plenty of imaging showing severe stenosis in asymptomatic patients, and conversely, minimal stenosis causing significant symptoms. The correlation between your actual symptoms and the imaging findings is what guides treatment.
Clinical examination is always first. I assess your walking pattern, balance, reflexes, strength in specific muscle groups, and sensation. I look for patterns that tell me which nerve roots are compressed. I also perform the Spurling test (cervical) or leg raise tests (lumbar) to reproduce or aggravate your symptoms, confirming the diagnosis.
MRI is the gold standard. It shows the spinal canal, nerve roots, discs, ligaments, and bone spurs with excellent detail. I can measure the degree of stenosis and see exactly which levels are affected. MRI also rules out other serious pathology like tumors or infections.
CT imaging is helpful when MRI isn't possible or when I need better bone detail for surgical planning. Sometimes a combination of MRI and CT gives me the clearest picture.
X-rays show degenerative changes and can reveal spondylolisthesis (vertebral slippage), which tells me about segmental stability.
For a deeper dive into stenosis anatomy and diagnosis, read my blog post on Understanding Spinal Stenosis.
Conservative Treatment: The First-Line Approach
The vast majority of stenosis cases respond well to non-surgical care, especially in earlier stages. My philosophy: reserve surgery for those who fail conservative therapy or have progressive neurological deficits.
Physical therapy is the cornerstone. A stenosis-specific PT program focuses on:
- Core stabilization: Strong deep abdominal and back extensor muscles support the lumbar spine and maintain good posture, which opens the spinal canal.
- Flexibility and stretching: Maintaining good hip and hamstring flexibility allows you to bend forward more easily, which you may instinctively do to relieve symptoms.
- Postural retraining: Many patients develop a stooped or forward-bent posture as they unconsciously try to open the canal. PT helps you maintain neutral posture during activities.
- Aerobic conditioning: Walking and low-impact exercise improve function and pain tolerance. Many patients walk better and farther as conditioning improves.
Most patients feel measurable improvement within 6–8 weeks of consistent PT, especially when combined with other measures.
Anti-inflammatory medications like NSAIDs can reduce inflammation around compressed nerves and improve your function enough to participate in PT. I use short courses of muscle relaxers when muscle guarding is limiting your activities.
Epidural steroid injections are particularly effective for stenosis. The steroid is delivered into the epidural space around the compressed nerve roots, reducing inflammation and providing relief for weeks or months. This window of relief allows PT to be more effective. I typically recommend up to three injections in a rolling 12-month period—beyond that, results usually diminish.
Activity modification is essential. I advise patients to:
- Avoid or modify activities that trigger symptoms (prolonged walking upright, hyperextension)
- Maintain activities that relieve symptoms (walking bent forward, cycling, swimming, elliptical)
- Take frequent short breaks rather than long walks
- Maintain core strength and flexibility through consistent PT
For more detailed guidance on non-surgical approaches, read my article on Spinal Stenosis Treatment.
Time and natural history matter too. Some stenosis stabilizes or progresses very slowly. Others worsen more rapidly. If you're managing well with conservative care, we continue that approach. But if symptoms progress or worsen, we reassess.
When Surgery Becomes Necessary
I recommend surgical decompression when:
- Conservative care fails: You've done 8–12 weeks of PT, received injections that have lost effectiveness, modified your activities, and you're still significantly limited in function and quality of life
- Progressive neurological deficit: Your leg weakness is worsening, or you're developing balance problems or gait disturbance, signaling imminent nerve damage
- Severe functional limitation: You cannot walk the distances you need to for work or life activities, causing real hardship
- Cauda equina syndrome: Bowel or bladder dysfunction, bilateral leg pain, or progressive bilateral weakness require urgent decompression—this is a surgical emergency
Surgical Options: Decompression, Fusion, or Both
Laminectomy is the fundamental decompression surgery. I remove the lamina—the back portion of one or more vertebrae—to directly open up the spinal canal and decompress the nerve roots. This is particularly effective for lumbar stenosis where the narrowing comes from bone spurs, thickened ligaments, and disc bulging encroaching from behind.
Many patients with single-level lumbar stenosis get excellent, durable relief from laminectomy alone. The nerve roots have room to move again, and symptoms resolve.
Laminectomy with fusion is my choice when the underlying stenosis involves or reveals instability—excessive motion or slippage between vertebrae. Fusion adds stability while decompression removes the sources of nerve compression. The combination addresses both problems.
Common scenarios for fusion:
- Spondylolisthesis with stenosis (vertebra slipped forward)
- Severe degenerative disc disease causing hypermobility
- Multi-level stenosis where decompression of all levels would remove too much stabilizing bone
- Prior spine surgery at the same level, where decompression alone might create instability
I perform minimally invasive fusion when possible, using pedicle screws and rod instrumentation with bone graft. This preserves muscle and ligament attachments, shortens operative time, and speeds recovery compared to traditional open techniques.
My technical approach draws on extensive training in both orthopedic spine and neurosurgical techniques. This gives me expertise in thorough nerve decompression and careful attention to protecting neural structures.
What to Expect From Decompression Surgery
The procedure is performed under general anesthesia. I position you prone, use real-time fluoroscopy for precise guidance, and make small midline incisions over the affected level(s). I carefully remove the lamina to open the spinal canal, remove bone spurs, decompress thickened ligaments, and visualize the nerve roots to ensure complete decompression. If fusion is indicated, I place pedicle screws and instrumentation.
Most single-level procedures take 1–2 hours. Many patients go home the same day; some stay overnight.
Recovery after minimally invasive laminectomy:
- Weeks 1–2: Rest, frequent short walks, pain management. Avoid bending.
- Weeks 2–6: Gradual activity increase under brace support if needed. PT can begin early.
- Weeks 6–12: Progressive strengthening, return to light work and activities.
- Months 3–6: Return to normal activities, full exercise, and full work duties.
For laminectomy-fusion, recovery is slightly longer (add 2–3 weeks to the timeline), but the principles are the same.
Serious complications from minimally invasive decompression are uncommon, but any surgery carries some risk. During your consultation, I'll discuss complications specific to your situation in detail.
Clinical Bottom Line
Spinal stenosis is extremely common, particularly with age. But common doesn't mean you have to live with pain and limitations.
Most cases respond beautifully to conservative care—PT, activity modification, and injections. For those whose stenosis doesn't respond or progresses, modern decompression surgery, performed with minimal-invasion techniques, provides excellent relief and returns you to function quickly.
My job is to accurately diagnose your stenosis, understand your goals and functional needs, and guide you through the treatment pathway—whether that's rehabilitation, injections, surgery, or combination therapy—that gives you the best outcome.
Next Steps
If you're experiencing leg pain with walking, numbness, weakness, or the classic "shopping cart sign," don't assume these symptoms are permanent. Many patients improve dramatically.
Schedule a consultation at my San Antonio or Houston office. We'll image your spine if needed, examine you carefully, and build a clear treatment plan based on your specific anatomy, symptoms, and goals.
Your spinal stenosis is unique to you. Your treatment plan should be too.
Common Symptoms
- Leg pain, heaviness, or fatigue that worsens with walking and improves with sitting ("shopping cart sign")
- Numbness or tingling in legs, feet, or buttocks
- Weakness in the legs or difficulty walking
- Balance problems or unsteadiness
- Pain that improves when leaning forward or bending at the waist
- Neck pain or stiffness (cervical stenosis)
- Weakness in the arms or hands (cervical stenosis, myelopathy risk)
- Radiating pain into the thigh or lower leg
Treatment Options
- Physical therapy with core stabilization and flexibility work
- Anti-inflammatory medications and pain management
- Epidural steroid injections to reduce nerve inflammation
- Activity modification and postural correction
- Laminectomy for canal decompression
- Laminectomy with fusion for unstable segments
- Lumbar fusion for symptomatic instability
Frequently Asked Questions
What is the 'shopping cart sign' in spinal stenosis?
The shopping cart sign is leg pain or heaviness that worsens with walking but improves when sitting or leaning forward. This classic pattern occurs because bending forward opens the narrowed spinal canal and relieves nerve pressure.
Does spinal stenosis get worse over time?
Stenosis can progress gradually, but it's often stable or progresses very slowly. Many people with imaging-confirmed stenosis remain asymptomatic for years. Regular monitoring and early conservative treatment help prevent or slow progression.
How effective is physical therapy for stenosis?
Physical therapy is highly effective for stenosis, especially in early stages. Programs emphasizing core strengthening, flexibility, and postural retraining help most patients improve walking tolerance and reduce symptoms within 6-8 weeks.
When should someone with spinal stenosis have surgery?
Surgery is considered after 8-12 weeks of unsuccessful conservative care, progressive neurological loss, or significant functional limitations affecting work or daily life. Cauda equina syndrome (bowel/bladder dysfunction) requires urgent decompression.
Can I get stenosis treatment in San Antonio?
Yes. Dr. Cyr specializes in spinal stenosis diagnosis and treatment at his San Antonio office (8401 Datapoint Drive). He offers minimally invasive decompression surgery when conservative care doesn't provide adequate relief.

