What Is a Spinal Fracture?
A spinal fracture is a break in one or more vertebrae—the bones that stack to form your spine. These fractures range from minor hairline breaks that heal with conservative care to severe, unstable fractures that require surgical stabilization. The mechanism of injury and the fracture pattern determine whether your spine can repair itself or needs surgical intervention.
As a fellowship-trained orthopedic spine surgeon, I evaluate every spinal fracture individually. The same condition in one patient may warrant surgery, while another patient can heal safely with bracing alone. This distinction is critical—getting it wrong risks permanent disability or chronic pain.
Common Types of Spinal Fractures
Compression Fractures
Compression fractures are the most common spinal fracture type, especially in older adults with osteoporosis. The front (anterior) portion of a vertebra collapses, often causing a wedge-shaped deformity. While a single compression fracture may cause only localized pain, multiple fractures lead to progressive height loss, kyphotic deformity (forward curvature), and functional decline.
Younger patients usually sustain compression fractures from high-energy trauma, but they often heal well with conservative treatment. Elderly patients with osteoporosis, however, may suffer fractures from minor falls or even spontaneous collapse.
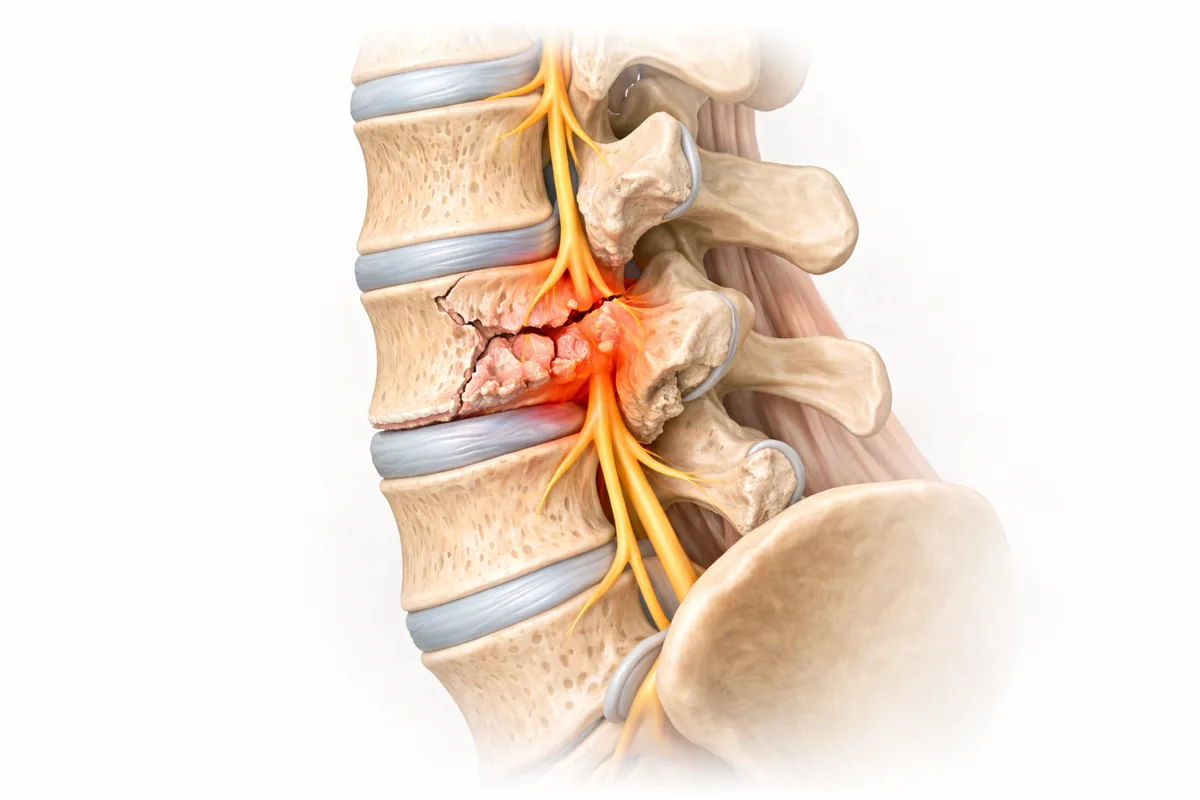
Burst Fractures
A burst fracture occurs when a vertebra is crushed from high-energy trauma—motor vehicle accidents, falls from height, diving injuries, or significant impacts. The vertebral body breaks in multiple directions, and bone fragments may retract into the spinal canal, potentially compressing the spinal cord or nerve roots. Burst fractures are more serious than simple compression fractures and frequently require surgical evaluation.
Flexion-Distraction Injuries
These fractures result from rapid flexion with distraction, classically seen in unrestrained drivers striking steering wheels in crashes or from lapses when seat belts are improperly positioned. The ligaments and bone may be disrupted across multiple spinal levels, creating an unstable injury that almost always requires surgery.
Fracture-Dislocations
The most severe and unstable spinal injuries combine a vertebral fracture with ligamentous disruption, causing vertebrae to shift and separate from their normal alignment. These injuries carry high risk of spinal cord damage and neurological deficit. They demand urgent surgical stabilization.
Why You Hurt: Mechanisms of Pain
Spinal fracture pain stems from multiple sources:
- Bone injury: Fractured vertebrae trigger inflammatory responses and pain signals at the injury site.
- Muscle spasm: Surrounding muscles contract protectively, creating secondary pain and stiffness.
- Nerve compression: Displaced bone fragments or swelling may compress nerve roots, causing radiating pain, numbness, or weakness.
- Ligament damage: Instability and inflammatory changes in supporting ligaments amplify pain during movement.
Acute fractures hurt severely because the injury is fresh and inflammation is high. Chronic pain after fracture often reflects muscle deconditioning, persistent inflammation, or unrecognized instability.
Diagnosis: How I Determine the Fracture Type and Stability
Accurate diagnosis is essential because treatment varies dramatically by fracture pattern.
Clinical Examination: I assess your pain location, mobility, neurological function, and mechanism of injury. Is your spine stable during movement, or do you have instability signs (midline tenderness, severe pain with flexion-extension)?
X-ray: Plain radiographs provide initial assessment of bone alignment, vertebral body height, and overall spinal curve.
CT Scan: CT offers superior detail of bone anatomy, revealing subtle fracture lines, fragment displacement, and canal compromise that plain films miss. For burst fractures, CT is essential.
MRI: MRI visualizes soft tissues—the spinal cord, ligaments, and intervertebral discs. If you have neurological symptoms or a severe burst fracture, MRI confirms whether the spinal cord is compressed or contused. This finding directly drives whether surgery is necessary.
When Surgery Is Needed
Not all spinal fractures require surgery. Stable compression fractures in younger patients, and even many in older patients, can heal with bracing and conservative care. However, surgery is indicated when:
- The spinal column is unstable (ligament disruption, fracture-dislocation)
- Bone fragments compress the spinal cord or nerve roots causing neurological deficit
- The fracture causes severe kyphotic deformity that will progress
- Conservative treatment has failed and chronic pain or instability persists
- Multiple-level fractures create cumulative instability
Surgical Treatment Options
Vertebroplasty and Kyphoplasty
For painful compression fractures without neurological compromise, vertebroplasty or kyphoplasty may be appropriate. These minimally invasive procedures inject cement directly into the fractured vertebra to stabilize it and reduce pain. Kyphoplasty includes a balloon step that restores vertebral height, reducing kyphotic deformity.
These techniques are most effective for acute compression fractures in patients with adequate bone quality. They are not suitable for burst fractures with canal compromise or fracture-dislocations.
Instrumented Fusion
Burst fractures, flexion-distraction injuries, and fracture-dislocations typically require surgical fusion. The approach depends on fracture location and pattern. I often combine anterior and posterior techniques to ensure complete stabilization.
My lumbar fusion approach includes decompression of any neural compression, realignment of the vertebral bodies, and instrumentation (screws and rods) to hold the spine stable during healing. Intervertebral cages or bone graft bridge the gaps and promote bone healing.
For unstable thoracic or lumbar injuries with neurological deficit, laminectomy-fusion removes posterior bone and ligament compressing the spinal cord, while instrumentation prevents recurrent instability.
Recovery and Rehabilitation
Post-operative recovery depends on fracture severity and surgical approach. Instrumented fusion typically requires 3-6 months for solid bone healing, with most patients returning to light activity within 2-3 months and full activity by 6 months.
Physical therapy is essential—it restores core strength, improves flexibility, and prevents secondary deconditioning. Many patients underestimate the value of rehabilitation and plateau in recovery. Committed therapy often determines whether you return to your pre-injury lifestyle or experience persistent limitations.
Why Choose Dr. Cyr for Spinal Fractures
Spinal fracture management demands precision. The wrong treatment delays healing, allows progression to instability, or leaves you with chronic pain. I bring fellowship-trained expertise and individualized judgment to every fracture case—matching the aggressiveness of treatment to your fracture's severity.
Whether your fracture heals with a simple brace or requires complex surgical stabilization, I'm committed to restoring your spinal stability and your quality of life.
Serving San Antonio and Houston with specialized spine care.
Related Conditions & Treatments
Contact us today to schedule your spinal fracture evaluation and get back to the activities you value.
Common Symptoms
- Acute or sudden severe back pain
- Limited spinal mobility and stiffness
- Visible deformity or loss of height
- Radiating pain or numbness (if nerve compression)
- Weakness or difficulty with movement
- Neurological symptoms (in severe cases)
Treatment Options
- Diagnostic imaging (X-ray, CT, MRI)
- Conservative bracing (for stable fractures)
- Vertebroplasty or kyphoplasty
- Instrumented fusion surgery
- Physical therapy and rehabilitation
Frequently Asked Questions
Do all spinal fractures require surgery?
No. Stable compression fractures, especially in younger patients, often heal well with conservative treatment and bracing. Surgery is reserved for unstable fractures, burst fractures with nerve compression, or progressive deformity.
How is spinal fracture stability determined?
Imaging (X-ray, CT, MRI) and clinical examination determine fracture stability. Unstable fractures involve ligament disruption or vertebral slippage. Dr. Cyr evaluates each fracture individually to match treatment to severity.
What is vertebroplasty or kyphoplasty?
These minimally invasive procedures inject cement into a fractured vertebra to stabilize it and reduce pain. Kyphoplasty includes a balloon step to restore height. They work best for painful compression fractures without nerve compression.
How long is recovery from spinal fracture surgery?
Recovery from instrumented fusion typically takes 3-6 months for bone healing, with return to light activity in 2-3 months and full activity by 6 months. Physical therapy is essential throughout recovery.
Can I get expert spinal fracture care in San Antonio?
Yes. Dr. Cyr, a fellowship-trained spine surgeon, evaluates and treats spinal fractures at his San Antonio office (8401 Datapoint Drive). He determines whether your fracture needs conservative or surgical care.

