About Lumbar Fusion
When lower back pain stems from instability, degeneration, or structural failure of the spine, fusion is often the definitive answer. Lumbar fusion creates a solid bone bridge between two or more vertebrae, eliminating painful motion at the affected segment and stabilizing the spine.
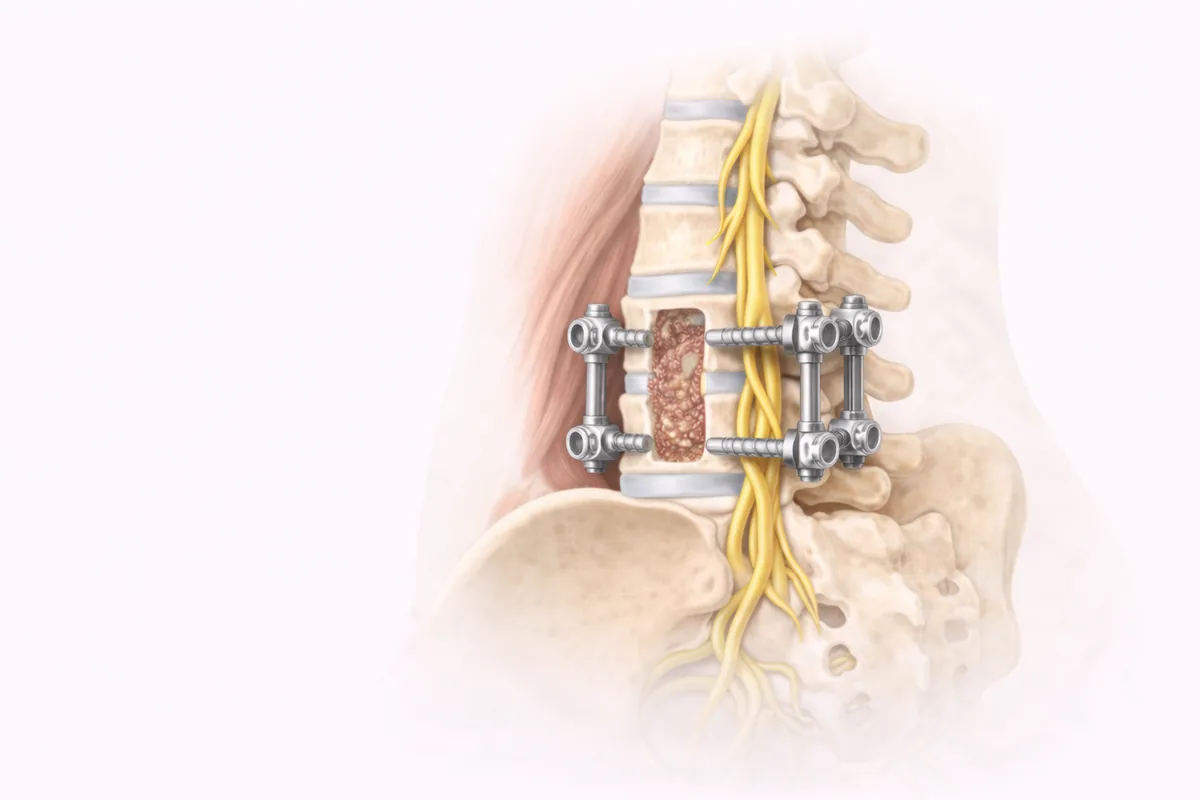
I perform percutaneous lumbar fusion—a technique that achieves excellent fusion outcomes with minimal trauma to surrounding muscles and soft tissues. Rather than large open incisions that cut through the paraspinal muscles, we work through small "keyhole" portals. Real-time fluoroscopy (live X-ray guidance) allows me to place pedicle screws with precision, then connect them with rods to create a rigid construct. Bone graft placed during surgery fuses the vertebrae over the following months—the same natural healing process that mends a broken bone.
My training as Chief of Air Force Spine Surgery combined with my Mayo Clinic fellowship in both orthopedic and neurosurgical spine techniques gives me the technical refinement to handle these complex cases. I've refined this approach over decades, achieving success rates of 90–95% for appropriately selected patients.
When Lumbar Fusion Is Recommended
Fusion is not the first step. I recommend conservative care—physical therapy, anti-inflammatory medication, and targeted injections—for most acute back pain. Fusion surgery becomes the right choice when mechanical or axial lower back pain persists despite these measures, or when your spine shows structural failure that demands stabilization.
Common indications I see in my San Antonio and Houston practices include:
Degenerative disc disease — When discs lose height and hydration, the joints become unstable and facet degeneration accelerates, causing grinding pain with movement or position change.
Spondylolisthesis — A vertebra slips forward on the one below, pinching nerves and destabilizing the spine.
Post-laminectomy syndrome — Back pain that develops after decompression surgery due to loss of spinal stability.
Traumatic fracture or instability — Severe injury or structural collapse that cannot heal on its own.
Scoliosis with mechanical pain — Abnormal curvature combined with degenerative changes causing severe pain.
The key: your pain must be mechanical in nature—worse with certain activities or positions, better with rest—and must not respond to at least three months of conservative therapy.
The Minimally Invasive Approach
This is where percutaneous fusion sets a new standard. Traditional open fusion requires a large midline incision and separation of the paraspinal muscles, leading to significant postoperative muscle pain and prolonged recovery.
With percutaneous technique, I make small incisions—often just one inch or less—through which specialized instruments and guides allow me to reach the pedicles (the bony bridges on the back of the vertebrae). Using real-time fluoroscopy for guidance, I insert pedicle screws into the vertebral bodies with millimeter precision. These screws are then connected by a titanium rod, creating a rigid fixation that prevents motion and allows fusion to occur.
If decompression is needed to address nerve compression, I may add interbody fusion by removing the disc and inserting a bone graft spacer or synthetic cage into the disc space. This expands the spinal canal and foramen, relieving pressure on neural elements.
The entire procedure typically takes one hour per level fused. Most patients go home the same day.
Advantages over open fusion:
- Minimal blood loss and smaller incisions mean less infection risk
- Preservation of muscle integrity shortens recovery significantly
- Less postoperative pain and faster return to normal activity
- Outpatient or short-stay hospitalization reduces healthcare costs
- Reduced scarring and tissue trauma
What to Expect
You'll be under general anesthesia. I position you prone (face down), sterilize and drape the surgical area, then make my small incisions over the pedicles. Using fluoroscopic guidance, I advance specialized instruments to create a pathway for the screws. Once both screws are in place and confirmed with imaging, I connect them with a rod and secure everything with minimal closure.
You'll feel immediate stability—no more hypermobility or painful shifting. If I've also performed interbody fusion, the bone graft begins its natural healing process right away.
Most patients wake in recovery within a couple of hours, receive pain management, and are discharged the same day with clear discharge instructions. You'll wear a lumbar brace for four to six weeks to support healing and remind you not to overextend.
Recovery and Rehabilitation
Lumbar fusion recovery is faster than you might expect, thanks to the minimally invasive approach.
First two weeks: Rest, frequent short walks (10 minutes twice daily), ice as needed, and oral pain medication. Avoid bending, twisting, and heavy lifting. Sleep on your back or side with pillow support.
Weeks 2–6: Continue bracing. Gradually increase walking distance. Begin gentle lumbar stabilization exercises as tolerated. No lifting more than 5 pounds. Avoid hills and uneven terrain.
Weeks 6–12: Brace can usually be discontinued. Physical therapy becomes more active—core strengthening, flexibility work, and functional retraining. Light work activities may resume around 4–6 weeks; full work duties depend on your job.
Months 3–12: Full bone fusion is still completing. Avoid heavy labor, high-impact sports, and contact sports during this period. Progressive resistance training under professional guidance is fine. Most patients report maximum pain relief and functional improvement by the 6-month mark, though fusion continues maturing to 12 months.
Long-term: Once fused, that segment will no longer move—period. Your adjacent segments may carry slightly more load over decades, a well-documented phenomenon. However, maintaining core strength, flexibility, and proper ergonomics minimizes the risk of future adjacent-level disease.
I encourage all my patients to stay active. Walking, swimming, core strengthening, and good body mechanics are your best insurance for long-term spine health.
Ready to discuss whether lumbar fusion is right for you? I offer consultations at both my San Antonio and Houston offices. We'll review your imaging, discuss your goals, and explore all options before surgery ever becomes the plan.
Schedule a consultation or call our office today.
When This Procedure Is Recommended
- Chronic mechanical lower back pain unresponsive to conservative treatment
- Spinal instability or degeneration of the lumbar discs or facet joints
- Spondylolisthesis (vertebral slippage)
- Degenerative disc disease with persistent pain
- Pain from traumatic spine injury or fracture
- Chronic pain from post-laminectomy syndrome
Surgical Techniques
- Percutaneous Lumbar Fusion with Pedicle Screws
- Transforaminal Lumbar Interbody Fusion (TLIF)
- Anterior Lumbar Interbody Fusion (ALIF)
- Posterior Lumbar Interbody Fusion (PLIF)
Frequently Asked Questions
How long does recovery from percutaneous lumbar fusion take?
Most patients go home the same day or after an overnight stay. You can return to light activities within 2–4 weeks and full work duties by 6–8 weeks. Fusion bone healing continues for 3–6 months.
What is the success rate of lumbar fusion surgery?
Dr. Cyr achieves success rates of 90–95% for appropriately selected patients using percutaneous minimally invasive techniques. Success means significant pain relief, improved function, and durability over time.
Will I be able to lift and exercise after lumbar fusion?
Yes, but with guidelines. Heavy lifting is restricted for 3–6 months during fusion healing. After full fusion, you can return to most activities including exercise, though very heavy labor is often discouraged to protect long-term spine health.
Why do some surgeons use percutaneous approach instead of open fusion?
Percutaneous fusion uses small incisions and preserves muscle integrity, resulting in less blood loss, reduced infection risk, and faster recovery compared to traditional open fusion that cuts through paraspinal muscles.
How long will a lumbar fusion last?
Once fused, that segment remains stable for life. The fusion is permanent. Adjacent segments may experience degenerative changes over decades, but maintaining core strength and proper mechanics minimizes this risk.

