Over my career as a Mayo Clinic-trained orthopedic spine surgeon, I've seen remarkable advances in how we treat spinal stenosis. Patients often ask me, "What's the newest treatment?" My honest answer: the newest technology is valuable, but precision surgical judgment remains the true gold standard.
Here's what I've learned about treating stenosis at every stage—and why one-size-fits-all approaches often fall short.
For an overview of what stenosis is and how it develops, see my post on Understanding Spinal Stenosis.
Understanding Spinal Stenosis Severity
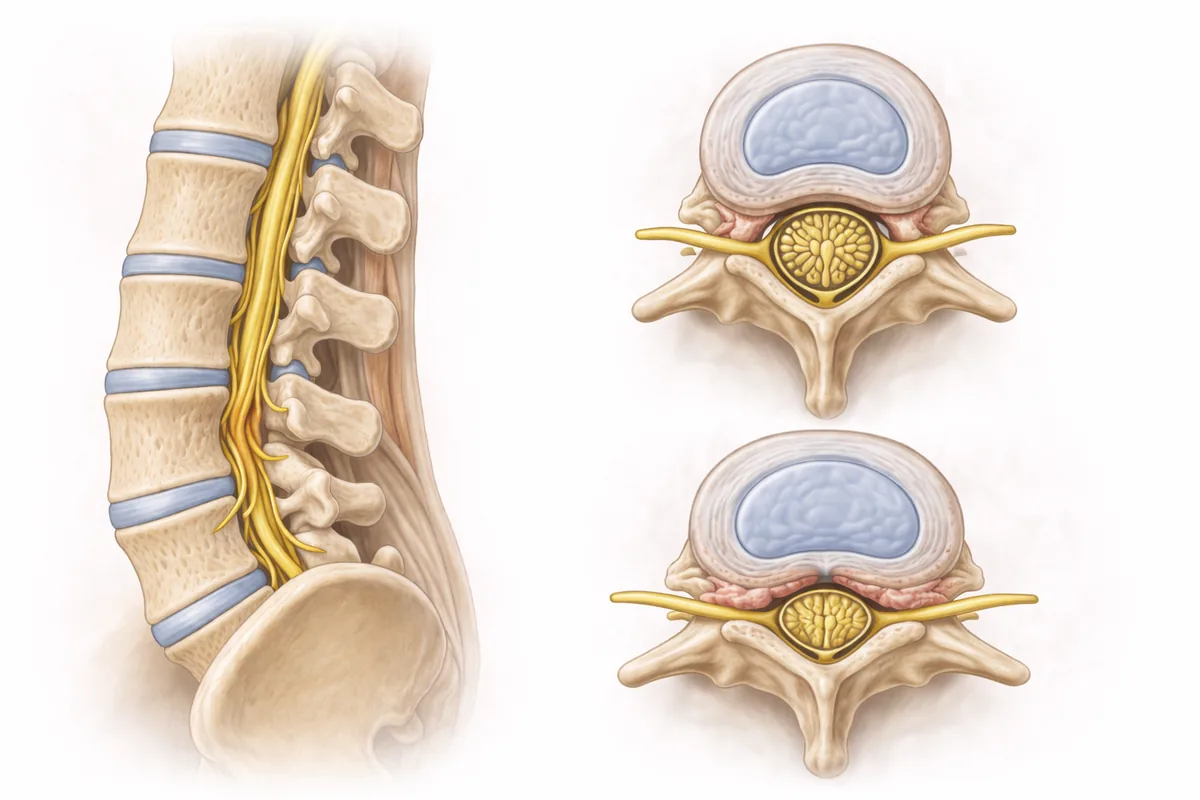
Spinal stenosis develops progressively. The vertebral canal narrows, reducing space for the spinal cord and nerve roots. Pain, numbness, weakness, and neurogenic claudication (leg pain with walking) are hallmark symptoms. But severity varies enormously from patient to patient.
I categorize stenosis into four distinct stages, each calling for different strategies:
Stage 1: Early Degeneration
At this stage, disc height is beginning to diminish and small bone spurs may appear. Most patients experience only mild symptoms—occasional stiffness, discomfort after activity, or positional pain.
My approach: Physical therapy, posture correction, and anti-inflammatory management almost always succeed here. Core strengthening and lifestyle modifications (ergonomic workplace setup, proper lifting mechanics) can halt progression. This is where conservative care shines.
Stage 2: Moderate Narrowing
The canal narrows more significantly. Patients report persistent pain, tingling, and numbness. Neurogenic claudication becomes evident—they walk a certain distance, then must sit or bend forward to decompress the nerves and continue. (Learn more about spinal stenosis symptoms and when to seek care.)
My approach: We escalate conservatively first. Continued physical therapy, targeted epidural steroid injections, and strategic pain management often provide lasting relief. Imaging becomes important to confirm the diagnosis and rule out other pathology.
Stage 3: Severe Stenosis
Here the canal is significantly compromised. Patients have frequent pain, noticeable leg weakness, and markedly reduced mobility. They may struggle with walking, standing, or simple daily activities.
My approach: This is where surgery enters the conversation. At this stage, conservative care typically plateaus. Minimally invasive decompression (through smaller incisions) often relieves compression and allows nerve healing. If imaging shows instability—ligament laxity or vertebral slipping—we may combine decompression with fusion to restore structural integrity.
Stage 4: Advanced Stenosis with Instability
The most severe cases combine profound canal narrowing with spinal instability. The vertebrae may be slipping (spondylolisthesis), or ligament destruction has compromised the spine's mechanical stability.
My approach: Here, fusion becomes essential. Decompression alone won't suffice if the spine is unstable. We must restore alignment and prevent future slipping. Advanced imaging (CT, dynamic MRI) guides surgical planning. Postoperative rehabilitation is critical to rebuild strength and proprioception.
Modern Treatment Options: Hype Versus Reality
The marketplace is flooded with new technologies. Endoscopic systems, laser decompression, interspinous spacers, motion-preservation devices—all have their place. But I've learned a hard lesson: newer doesn't mean better for every patient.
Minimally Invasive Laminectomy and Laminotomy
These approaches use smaller incisions than traditional open surgery, reducing muscle trauma and shortening recovery. I regularly perform minimally invasive decompression, and when the anatomy is suitable, the results are excellent. Patients recover faster, return to activity sooner, and experience less postoperative pain.
My philosophy: MIS techniques are tools that enhance outcomes when applied judiciously. The principles remain unchanged: identify the source of compression, remove it carefully, and preserve spinal stability. Technique and judgment matter more than incision size.
Endoscopic Spine Surgery
Endoscopic systems use tiny cameras and instruments to remove stenotic tissue under direct visualization. For select cases with lateral recess stenosis or foraminal narrowing, this can be elegant and effective.
The caveat: Endoscopy excels at decompression but offers limited options if fusion is needed. It's not a replacement for traditional approaches in unstable spines. I use endoscopy when the anatomy fits and decompression alone is sufficient.
Interspinous Spacers
These small devices sit between spinous processes to maintain canal opening and reduce extension-based symptoms. They can help patients with neurogenic claudication who have failed conservative care.
Realistic expectations: Spacers work best in early-to-moderate stenosis without severe facet arthropathy or instability. They're not a cure; they're a bridge—sometimes buying time, sometimes providing durable relief. But they won't help if the real problem is instability.
Gold Standard: Decompression with Fusion
When stenosis involves instability, nothing beats the combination of decompression (freeing the nerves) and fusion (restoring stability). Whether I'm performing laminectomy with fusion or lumbar fusion, the principle is consistent: remove what's compressing, then stabilize what's unstable.
This approach has decades of evidence. It works because it addresses both the symptom (nerve compression) and the underlying problem (segmental instability).
Why "Newest" Often Isn't "Best"
I trained at Mayo Clinic in an era when surgical innovation was (and still is) relentless. I've seen trends come and go. Some innovations genuinely improve outcomes. Others are marketed brilliantly but offer marginal benefit at premium cost.
Here's what 20+ years of complex spine surgery has taught me:
- Technology enhances judgment; it doesn't replace it. A great surgeon with older instruments often outperforms a mediocre surgeon with fancy equipment.
- Precision tailoring beats one-size-fits-all. Two patients with identical imaging may need entirely different treatments based on age, comorbidities, activity level, and goals.
- Instability is the game-changer. Once a spine is unstable, no amount of minor decompression or spacer technology will provide lasting relief. Fusion becomes necessary.
- Recovery and rehab matter as much as the surgery. I can execute a perfect fusion, but if the patient doesn't commit to structured physical therapy, core strengthening, and posture retraining, outcomes suffer.
My Approach: San Antonio and Houston
At my practices in San Antonio and Houston, I tailor stenosis treatment to each patient's unique presentation. If conservative care can solve the problem, that's my first choice. If surgery is needed, I choose the approach—whether traditional open fusion, minimally invasive decompression, or a hybrid strategy—that best fits your anatomy, your stability, and your life goals.
I don't use technology because it's new. I use it because it serves the patient better.
If you're struggling with spinal stenosis and want a surgeon's honest assessment of your options, I'm here to help. Contact my office in San Antonio or Houston to schedule your consultation.
Related Reading:
- Understanding Spinal Stenosis
- Spinal Stenosis: Symptoms & Treatment
- Sciatica & Nerve Pain
- Endoscopic Spine Surgery
Dr. Steven Cyr is a board-certified orthopedic spine surgeon with fellowship training from Mayo Clinic. He specializes in complex spine reconstruction and has performed thousands of minimally invasive and open spine procedures.
Frequently Asked Questions
What is neurogenic claudication and how does it differ from regular leg pain?
Neurogenic claudication is leg pain or cramping that develops with walking or standing due to nerve compression in the spinal canal. Unlike vascular claudication, symptoms typically improve quickly when you sit or bend forward, which decompresses the nerves.
Can epidural steroid injections treat spinal stenosis permanently?
Epidural injections reduce inflammation and nerve irritation, providing relief that can last weeks to months. They're not a permanent cure, but they can give conservative care time to work and sometimes provide lasting symptom control without surgery.
What is minimally invasive laminectomy and how is it different from open surgery?
Minimally invasive laminectomy uses smaller incisions and specialized instruments to remove bone and ligament compressing the nerves, reducing muscle trauma compared to open surgery. Recovery is typically faster and postoperative pain is less.
When is fusion necessary along with decompression for stenosis?
Fusion is combined with decompression when the spine is unstable—typically indicated by vertebral slipping (spondylolisthesis), significant ligament damage, or instability seen on imaging. Decompression alone won't provide lasting relief in unstable spines.
Can I get minimally invasive spinal stenosis surgery in San Antonio or Houston?
Yes. Dr. Cyr performs both traditional and minimally invasive stenosis treatments at his San Antonio and Houston practices, tailoring the approach to each patient's anatomy and clinical presentation.

